Back to: Trial Questions
Anterior (Smith-Robinson) approach (to subaxial spine)
- Indication
- Exposes C2-T1
- Anterior cervical discectomy + fusion
- Anterior cervical corpectomy + fusion
- Infection, Odontoid fracture
- Position
- Supine, 30° head-up with sandbag in interscapular region to extend neck
- Neck rotated slightly to contralateral side
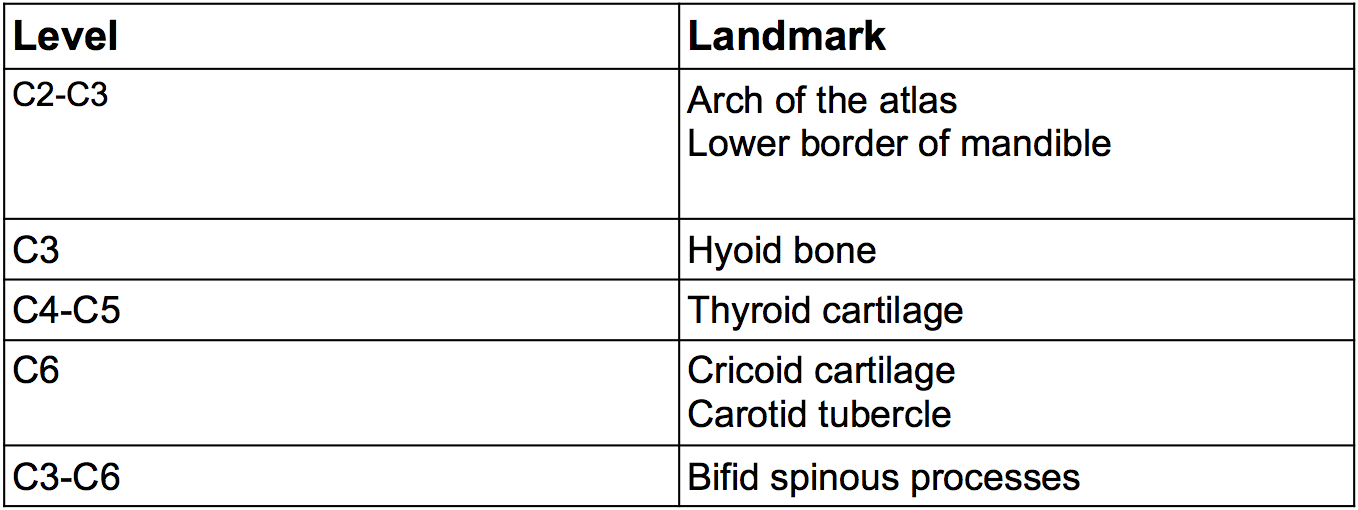
- Landmarks
- See table
- Incision
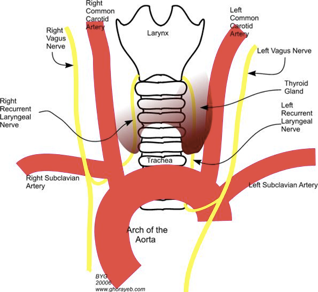
- Right or left side (below C5, L-side safer in avoiding inadvertent injury to RLN
- Transverse incision over ant. Sternocleidomastoid
- Can use oblique incision
- Internervous plane
- No true INP
- Superficial dissection
- Platysma, in-line with fibres
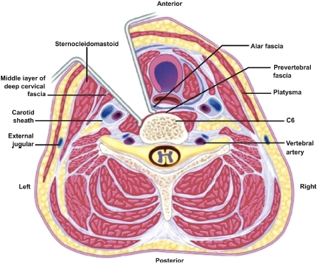
- Deep dissection
- Incise deep cervical fascia at ant. Border of Sternocleidomastoid
- Sternocleidomastoid muscles laterally, strap muscles medially (sternohyoid/sternothyroid)
- Retract SCM laterally with carotid sheath laterally
- Retract strap muscles with trachea & oesophagus medially
- Expose prevertebral fascia + longus colli muscles- retract laterally with incised ALL
- Be aware of sympathetic chain (lies on LC lateral to VB)
- Divide prevertebral fascia longitudinally in the midline to expose disc + vertebral body
- K-wire/clip & lateral x-ray to confirm level
- Risks
- Superior thyroid artery above C4, Inferior thyroid artery below C6, may need ligating
- Recurrent Laryngeal Nerve (more so on the right)
- Carotid sheath (encloses common carotid artery, internal jugular vein and vagus nerve)
- Thoracic duct below C7 in Left-sided approach
- Sympathetic nerves + stellate ganglion – damage causes Horners syndroome (ptosis, anhydriosis, miosis, enophthalamos)